
An insole can change how your foot contacts the ground, how quickly the arch moves, and where pressure is concentrated inside the shoe. Those small changes can influence the angle and timing of motion farther up the leg. That does not mean every painful knee begins in the foot. It means the foot is one of several places where daily load can be adjusted.
The most useful question is therefore not “What is the best insole?” but “What problem am I asking the insole to solve?” A person whose arch collapses inward needs something different from a person with a rigid high arch who simply wants more impact comfort on concrete floors.
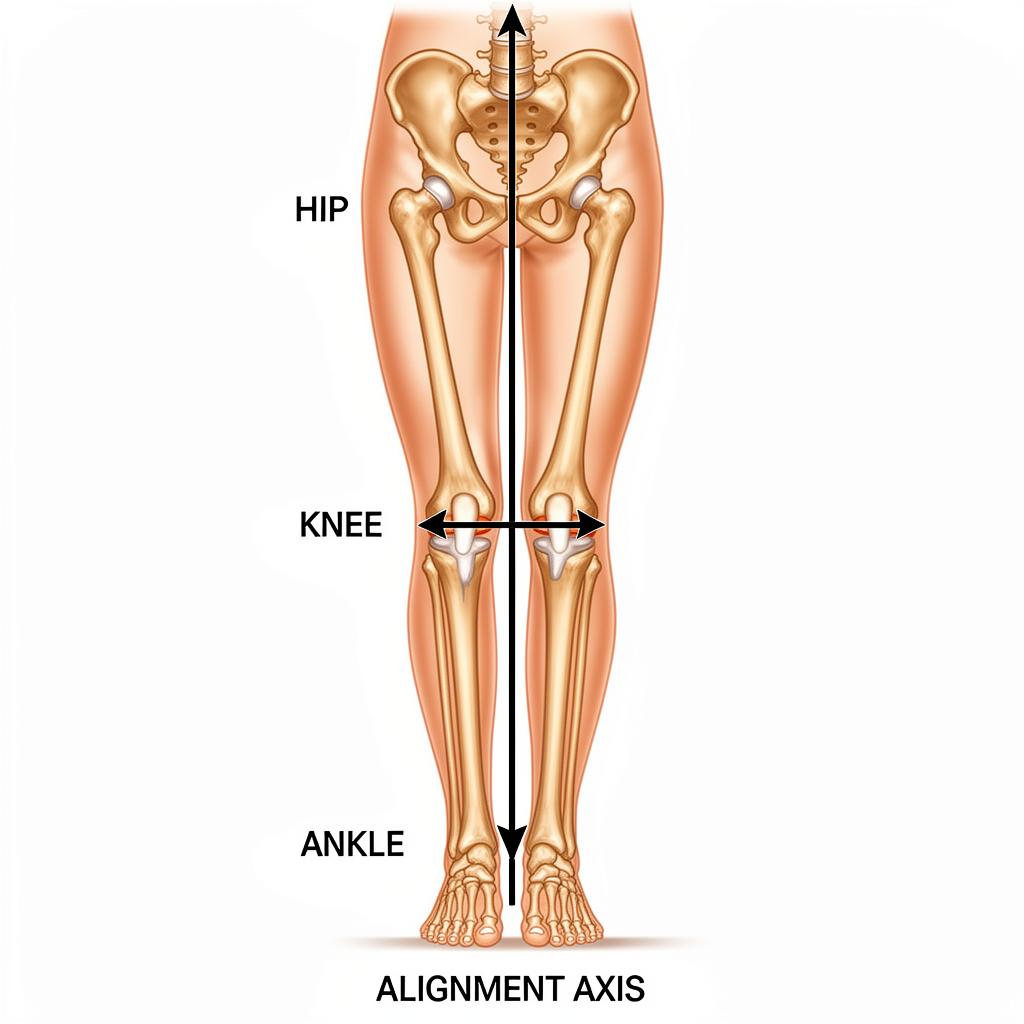
How the Foot–Ankle–Knee Chain Works
During a step, the foot first accepts load, then adapts to the surface, and finally becomes a firmer lever for push-off. Some inward roll — pronation — is normal. The concern is not pronation itself, but motion that is excessive for the person, poorly controlled, or combined with a shoe that no longer provides a stable platform.
When the arch drops and the ankle rolls inward, the shin can rotate inward with it. The thigh and kneecap must then manage a slightly different line of force. In some people, especially those with front-of-knee discomfort, changing that chain can make walking or running feel easier. Current best-practice guidance for patellofemoral pain includes prefabricated foot orthoses as a possible supporting intervention for selected people, usually combined with education and exercise rather than used as a stand-alone fix.
A useful expectation
An insole is a load-management tool, not a diagnosis or a cure. A successful trial may mean you can walk longer with less irritation, finish a work shift more comfortably, or recover more easily — not that every knee symptom disappears.
Match the Insole to the Pattern
| Insole type | Best starting use | What to feel for | Common mistake |
|---|---|---|---|
| Structured arch support | Arch collapse, inward shoe lean, front or inner knee discomfort during walking | Firm contact under the arch without a sharp pressure point | Buying the highest arch because it looks more supportive |
| Cushioning / impact control | Hard floors, long standing, rigid or higher arches | Softer landing without the heel sinking or wobbling | Choosing thick foam that makes the shoe unstable |
| Deep heel cup | A heel that shifts inside the shoe or needs a more centered base | Secure heel placement with no rubbing at the edge | Using it in a shoe whose heel counter is already collapsed |
| Wedge or posted orthotic | A specific load-shifting goal identified by a professional | A subtle change, not a dramatic tilt | Guessing the direction and moving pressure to the wrong area |
1. Structured Arch-Support Insoles
These use a semi-rigid shell or firmer foam under the midfoot. They are the most logical retail category when the arch visibly flattens, the ankle rolls inward, or the shoe develops an inward lean. Support should feel broad and steady. A hard ridge pressing into one small spot is not “good pain”; it is usually the wrong arch position or height.
2. Cushioned Insoles
Cushioning may be more relevant when the foot is relatively stable but impact feels harsh — for example, during long shifts on tile, concrete, or warehouse flooring. The goal is not maximum softness. Very thick gel or memory foam can raise the foot, reduce space around the toes, and create side-to-side movement. Look for controlled cushioning with a stable heel base.
3. Heel Cups and Heel-Focused Inserts
A deep heel cup can improve how the rear of the foot sits inside the shoe. This may help when the heel slides, the rearfoot feels unstable, or cushioning has flattened. A heel-only insert also changes how the shoe fits, so check that it does not push the heel upward and cause rubbing at the collar.
4. Wedges and Posted Orthotics
A wedge intentionally shifts pressure toward one side. That can be useful for a specific mechanical or knee-compartment goal, but it is not a neutral product. Because the direction matters, this is the category most worth discussing with a podiatrist, physical therapist, or other qualified clinician.
Five Clues Your Footwear Is Worth Investigating
None of the following proves that the foot is the source of knee discomfort, but several clues together make a structured footwear test more reasonable:
- Your shoes lean inward or the midsole looks more compressed on one side.
- Your arches appear lower when standing than when sitting.
- Discomfort builds with walking or standing on hard surfaces and improves after changing shoes.
- One pair of shoes consistently feels better than another despite similar activity.
- The heel counter, outsole, or insole is visibly worn and no longer holds the foot securely.

How to Choose a Pair Without Overspending
Start with the shoe, not the insert
Remove the original liner and inspect the midsole and heel counter. If the shoe twists easily, leans, or has compressed asymmetrically, a premium insert will sit on an unstable base. Replace the shoe first. Our running-shoe guide explains the broader footwear decision.
Match the volume of the insert to the shoe
Running shoes often accept a full-length replacement insole. Dress shoes and low-volume trainers may not. Whenever possible, remove the original liner rather than stacking inserts. Stacking raises the heel and forefoot, crowds the toes, and may create a new pressure problem.
Choose the closest arch height, not the strongest label
Low, medium, and high arch options refer to geometry, not quality. The right insert makes contact without forcing the foot outward or creating numbness. If you cannot test in store, prioritize retailers that allow a genuine fit trial.
Check width and trim lines
Place the old liner over the new one and trace it before trimming. Cut conservatively in small stages. The insert should lie flat from heel to toe without buckling, curling, or leaving the heel perched on an edge.

A Sensible Two-Week Adaptation Plan
- Days 1–2: Wear the inserts for one to two hours during ordinary activity.
- Days 3–5: Increase to half a day if there is no rubbing, numbness, or new joint discomfort.
- Days 6–9: Use them through a normal work or walking period, but avoid testing them for the first time during a long run or trip.
- Days 10–14: Compare end-of-day knee and foot comfort with your previous footwear routine.
Mild awareness under the arch can be normal at first. Sharp pressure, blisters, tingling, or a new pain pattern is a reason to stop and reassess the fit. Keep your old liners until the trial is complete.
Do not change everything at once
New shoes, new insoles, a new running surface, and a major mileage increase in the same week make it impossible to know what helped or hurt. Change one major variable, observe, then progress.

Support the day — then build a calmer evening routine
A well-fitted insole can change how load reaches the knee during movement. FlexiKnee is designed for a separate role: a convenient warmth, red-light, and vibration routine after the day is done.
View Full Product DetailsSport and Running: What Changes?
For running, court sports, or gym use, the insert must stay flat during faster movement and should not make the heel unstable. Test it first during a short, familiar session. Athletes with a rigid high arch may prefer impact control; those whose feet roll inward may prefer a more structured platform. Neither category automatically prevents injury.
When returning to activity, pair the footwear change with gradual load progression. Sudden increases in distance, hills, speed work, or lower-body volume can exceed tissue tolerance regardless of the insert. For a broader plan, see how to strengthen your knees and post-workout knee recovery exercises.
When Over-the-Counter Insoles Are Not Enough
Consider a professional assessment when the feet are markedly different, symptoms persist despite a careful footwear trial, you have diabetes or reduced foot sensation, there is recurrent skin breakdown, or pain follows an injury. Visible swelling, locking, repeated giving way, night pain, fever, or inability to bear weight also falls outside a simple insole experiment.
A clinician can look at the entire chain — foot mobility, ankle range, hip control, strength, training load, and the knee itself. Sometimes the best recommendation is a custom device. Sometimes it is a different shoe, a strengthening plan, or no orthotic at all.
Bottom Line: The Best Insole Is the One That Solves a Defined Problem
Choose structured support for excessive collapse, controlled cushioning for impact comfort, a secure heel cup for rearfoot stability, and professional guidance before experimenting with corrective wedges. Fit the insert to a stable shoe, adapt gradually, and judge the result during the activities that usually provoke discomfort.
Evidence supports foot orthoses as a useful option for selected knee-pain presentations, but not as a universal cure. The strongest plan still combines sensible footwear, progressive activity, and the muscle capacity to control the knee over time.
Sources and Further Reading
- Best practice guide for patellofemoral pain, British Journal of Sports Medicine (2024)
- International Patellofemoral Pain Research Retreat consensus statement on exercise and physical interventions (2018)
- Clinical review of common knee pain presentations and conservative management (2023)
This guide is educational and does not diagnose the cause of knee pain. Product selection should be individualized, particularly when symptoms are persistent, severe, or associated with swelling, instability, or injury.


